Triple-negative breast cancer and several other hard-to-treat tumors may have found an unlikely weak spot. It involves the same inflammatory pathway long targeted by a common asthma drug.
A Northwestern Medicine team reports that tumors can exploit a molecule called CysLTR1 to turn neutrophils, some of the body’s most common white blood cells, into cancer helpers. In mouse models and human tissues, blocking that pathway slowed tumor growth. It also improved survival and helped restore the immune system’s ability to respond to immunotherapy.
The work, published in Nature Cancer, centers on a receptor better known in asthma clinics than oncology labs. CysLTR1 helps mediate inflammation, and drugs that block it, including montelukast, have been prescribed for decades for asthma and allergies. In the new research, that same receptor emerged as a key control point in how tumors build an immune-suppressive environment.
“When we turned off this switch, either genetically or with existing drugs, we not only slowed tumor growth, but also helped the immune system recover its ability to fight the cancer,” said senior author Dr. Bin Zhang, the Johanna Dobe Professor of Cancer Immunology at Northwestern University Feinberg School of Medicine.
The findings suggest that an already approved drug could one day be tested as a partner to immunotherapy. This is especially true in cancers where checkpoint inhibitors often fall short.
They were recruiting it.
The Northwestern group found that tumors increase a population of neutrophils that act less like infection fighters and more like bodyguards for cancer. These cells belong to a broader class of suppressive myeloid cells that can shut down T cells. In addition, they support tumor growth and help cancers resist treatment.
What stood out was how tightly this process tracked with CysLTR1. Across multiple datasets, the receptor repeatedly appeared in tumor-associated myeloid cells. Follow-up experiments showed that its expression was especially high in tumor-infiltrating neutrophils and in neutrophils from several tumor models. These models included triple-negative breast cancer, melanoma, ovarian cancer, colon cancer and prostate cancer.
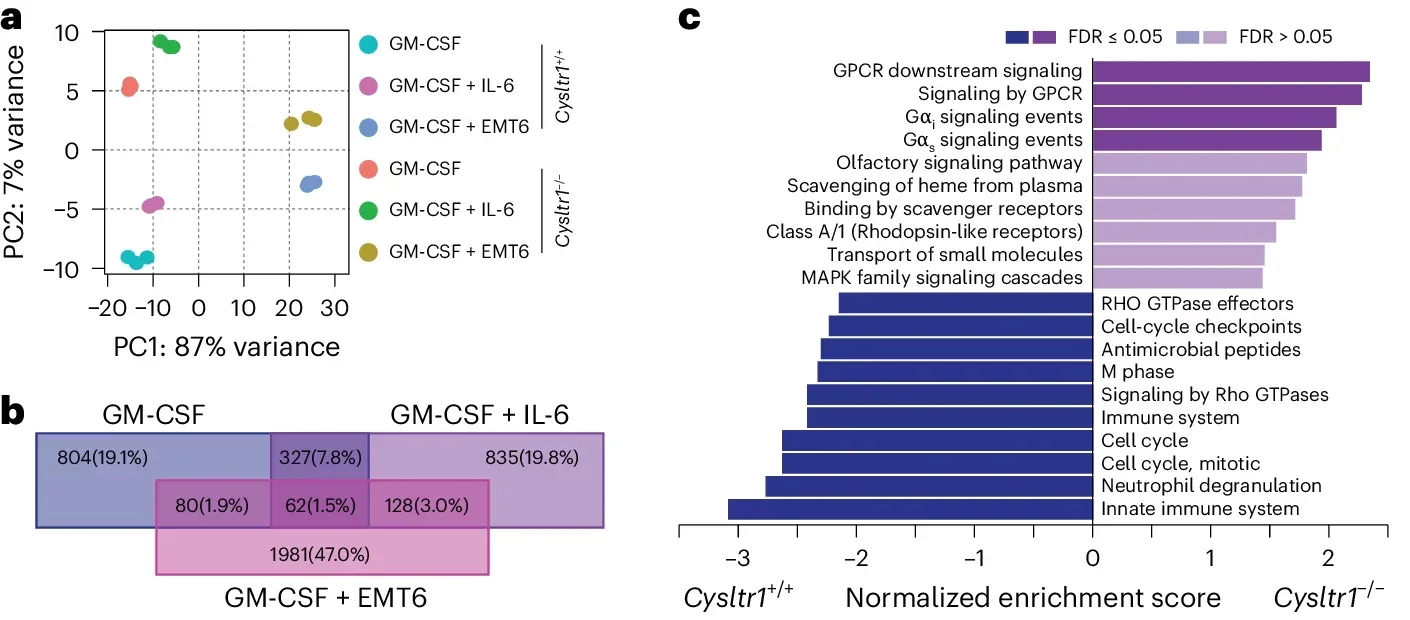
As tumors grew, the number of circulating neutrophils carrying CysLTR1 also rose, with even greater enrichment inside tumors. The signal was not static. Instead, it strengthened during tumor progression and appeared linked to inflammatory factors in the tumor environment. These included GM-CSF, G-CSF and IL-6, along with cysteinyl leukotrienes such as LTD4.
That matters because neutrophils are abundant, fast-moving and often overlooked in discussions of cancer immunotherapy, which usually focus on T cells. However, this study argues that the behavior of neutrophils may help decide whether those T cells ever get a fair chance.
When the team genetically removed CysLTR1 in mice, or blocked it with montelukast, tumors grew more slowly and animals lived longer. Those effects appeared in several models, including EMT6 and E0771 breast tumors, CT26 tumors and YUMMER1.7 melanoma. Furthermore, montelukast also suppressed spontaneous mammary tumors in an FVB-MMTV-PyMT model.
The change was not simply a loss of neutrophils. It was a change in what those cells became.
Without CysLTR1, neutrophils matured differently, accumulated less in bone marrow, spleen and tumors, and showed fewer features linked to immune suppression. At the same time, macrophages and dendritic cells rose modestly. The results pointed to a deeper rewiring of emergency myelopoiesis. This is the inflammatory process that shifts blood cell production toward tumor-supporting myeloid cells.
“Importantly, instead of simply removing these harmful white blood cells, we were able to reprogram them into cells that support immune attack,” Zhang said. “That means we’re not just targeting the cancer, we’re re-training one type of abundant immune cells in the body to fight the tumor again.”
The immune consequences were striking. Tumors lacking this CysLTR1-driven neutrophil program had more infiltrating CD4 and CD8 T cells, fewer regulatory T cells and less evidence of T cell exhaustion, including lower PD1 and TIM3 expression. Meanwhile, neutrophils from those tumors were less able to suppress T cell proliferation and, in some experiments, showed stronger antigen-presenting features.
When researchers depleted CD8 T cells, the survival advantage disappeared. That helped confirm that the tumor control seen after blocking CysLTR1 depended on restoring a stronger anti-cancer T cell response.
The study digs into the biology behind that shift.
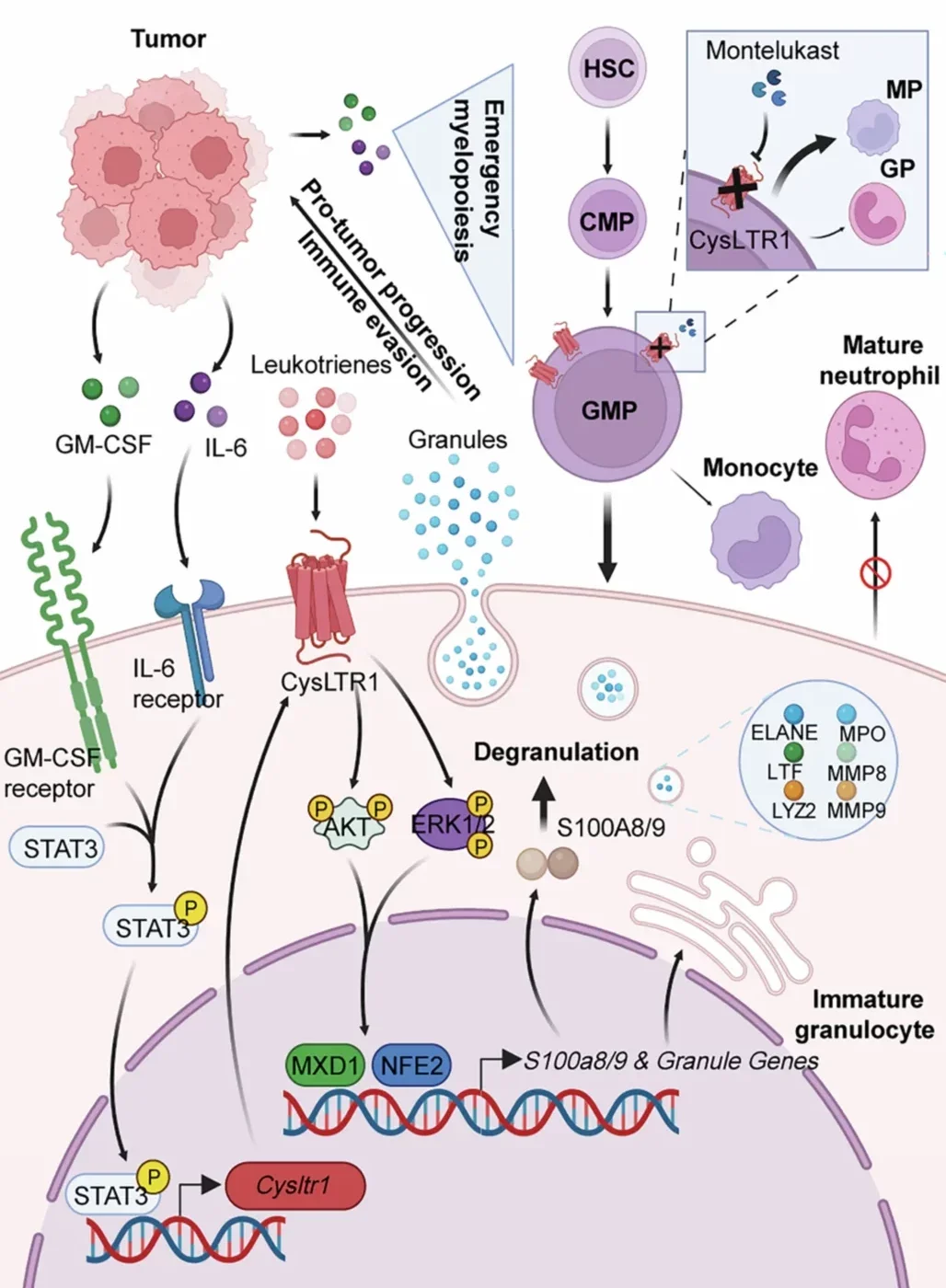
CysLTR1 appears to control how neutrophils mature and how they load up their internal granules, packets of enzymes and proteins that can promote tumor invasion, suppress immunity and help build neutrophil extracellular traps, or NETs. In the experiments, loss of CysLTR1 reduced NET formation and lowered levels of granule-related molecules such as MPO and S100A8/9.
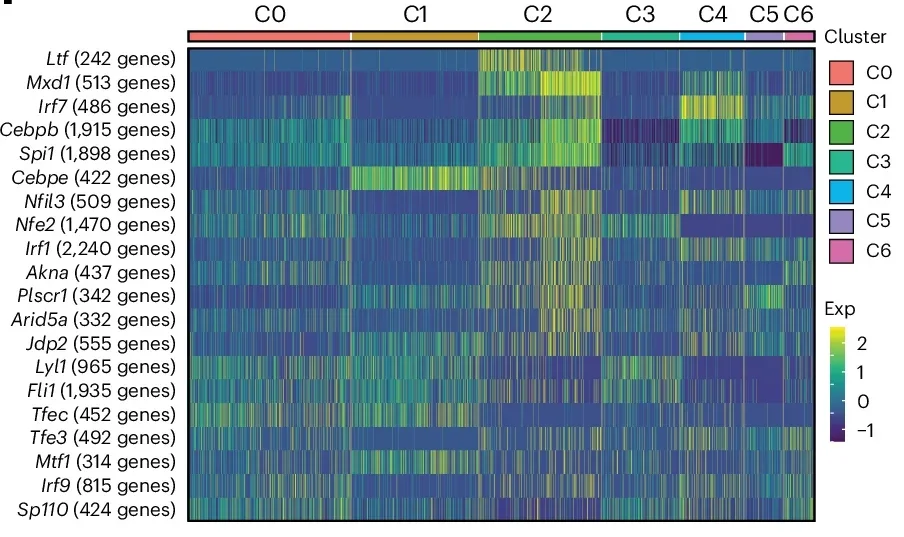
The team traced that program through a chain of molecular signals. Tumor-linked inflammatory cytokines, especially GM-CSF and IL-6, boosted CysLTR1 expression. STAT3 helped drive that increase by binding to the receptor’s promoter. Downstream, CysLTR1 activated AKT and ERK signaling, which in turn supported transcription factors including MXD1 and NFE2. Those factors helped switch on genes involved in neutrophil granule synthesis and suppressive behavior.
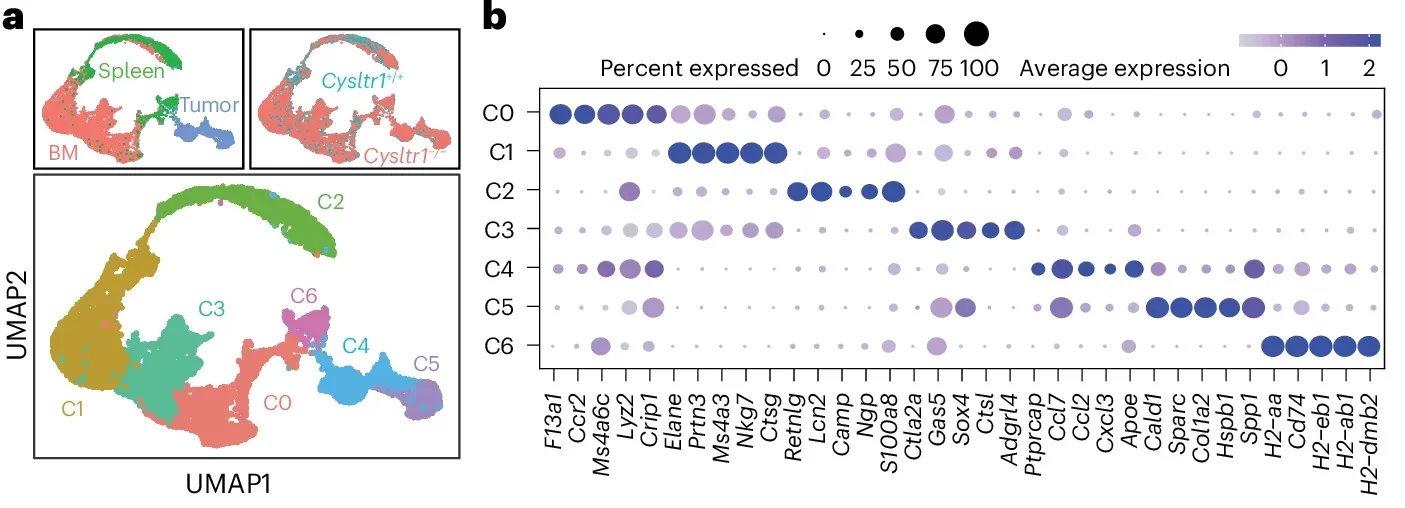
Single-cell RNA sequencing added another layer. It showed that neutrophils did not form one uniform population. Instead, they spread across several transcriptional clusters, with some more mature and suppressive, and others more tied to antigen presentation and immune activation. As a result, cells lacking CysLTR1 were pushed away from the suppressive states and toward more immunostimulatory ones.
That pattern held up in human material as well. In human peripheral blood cells, knocking down CYSLTR1 reduced neutrophil differentiation, lowered MPO and S100A8/9 expression, and weakened the cells’ ability to suppress CD8 T cells. Similarly, effects appeared in cells from people with ovarian cancer and with montelukast treatment.
In triple-negative breast cancer tissues, CD15+CD11b+ neutrophils expressing CysLTR1 also showed higher S100A9 intensity than their CysLTR1-negative counterparts.
Anti-PD1 treatment alone had little effect in one breast tumor model. But once CysLTR1 was removed, or montelukast was added, tumors became sensitive to the therapy.
The same combination effect showed up beyond breast cancer, including prostate, melanoma and ovarian tumor models. Public cancer datasets pointed in the same direction. Higher CYSLTR1 activity tracked with worse overall survival across multiple tumor types, while lower expression was associated with better survival and better responses to immune checkpoint blockade in several immunotherapy cohorts.
The research has limits. Much of the mechanistic work was done in mice, cell systems and public datasets. Therefore, the authors say the next step is to confirm the pathway in patients, identify who is most likely to benefit, work out the best drug combinations and move into carefully designed clinical trials.
Still, the practical appeal is obvious. Montelukast and other CysLTR1 blockers are already FDA-approved, which could lower the barrier to testing.
“We may be able to quickly and safely test it in cancer patients to improve immunotherapy. Especially in aggressive cancers, like triple-negative breast cancer, where new options are urgently needed,” Zhang said.
This work suggests that resistance to immunotherapy may depend not only on exhausted T cells, but also on how tumors reshape neutrophils before those T cells even act.
By blocking CysLTR1, researchers may be able to disarm a tumor-supporting arm of inflammation and make checkpoint drugs work better in cancers that usually resist them.
Because montelukast is already widely used, the findings open a relatively direct path toward clinical testing. Still, patient studies will have to show whether the same neutrophil rewiring seen in the lab can improve outcomes in real tumors.
Research findings are available online in the journal Nature Cancer.
The original story “Common asthma drug slows tumor growth and helps the immune system recover” is published in The Brighter Side of News.
Like these kind of feel good stories? Get The Brighter Side of News’ newsletter.
The post Common asthma drug slows tumor growth and helps the immune system recover appeared first on The Brighter Side of News.


Leave a comment
You must be logged in to post a comment.