Some of the smallest residents in an infant’s gut may be doing far more than anyone realized.
Two linked studies published in Nature Communications suggest that fungi, long overshadowed by bacteria in microbiome research, may help shape how a child’s immune system develops in the first months of life. In particular, the work points to a fungal group called Malassezia as a possible player in immune dysregulation tied to eczema, food allergy, and allergic asthma.
That matters because pediatric allergic diseases are already common, and still rising.
“Hundreds of millions of children worldwide are affected by allergic diseases, and the number is growing,” said Dr. Stuart Turvey, senior author of one of the studies, investigator at BC Children’s Hospital Research Institute, and professor of pediatrics at the University of British Columbia. “A better understanding of what gives rise to these conditions and how we can prevent them would have an enormous benefit for children around the globe.”
For years, microbiome science has focused mainly on bacteria. These two studies shift attention to the mycobiome, the fungal side of the gut ecosystem. Furthermore, they suggest it may be especially important during infancy, when immune development is still taking shape.
Turvey and colleagues used data from the CHILD Cohort Study to examine how fungal populations change during the first year of life. Their team analyzed 2,256 samples from 1,409 participants. In doing so, they found that fungal species followed distinct developmental paths.
Among the main trends, fungi from the Saccharomycetaceae family increased steadily over the first year. In contrast, Malassezia moved in the opposite direction.
That pattern mattered. The researchers found that different frequencies of certain fungal groups were associated with later immune-related conditions. Infants with more Malassezia, for example, were more likely to go on to develop atopic dermatitis.
The findings do not show that the fungus alone causes disease in children. But they do suggest that fungal profiles in infancy may serve as early markers of how the gut ecosystem is maturing. In addition, they raise the question of whether that process is getting off track.
Recent work had already linked persistent Malassezia colonization to delayed fungal maturation and increased risk of atopic dermatitis. The new analysis strengthens that picture by placing fungi more firmly inside the story of early immune development.
The second study, led by Dr. Marie-Claire Arrieta of the Snyder Institute for Chronic Diseases and the Alberta Children’s Hospital Research Institute at the University of Calgary, tackled the question from another angle. Instead of starting with disease associations, the team looked at what happens to the infant gut after antibiotic treatment.
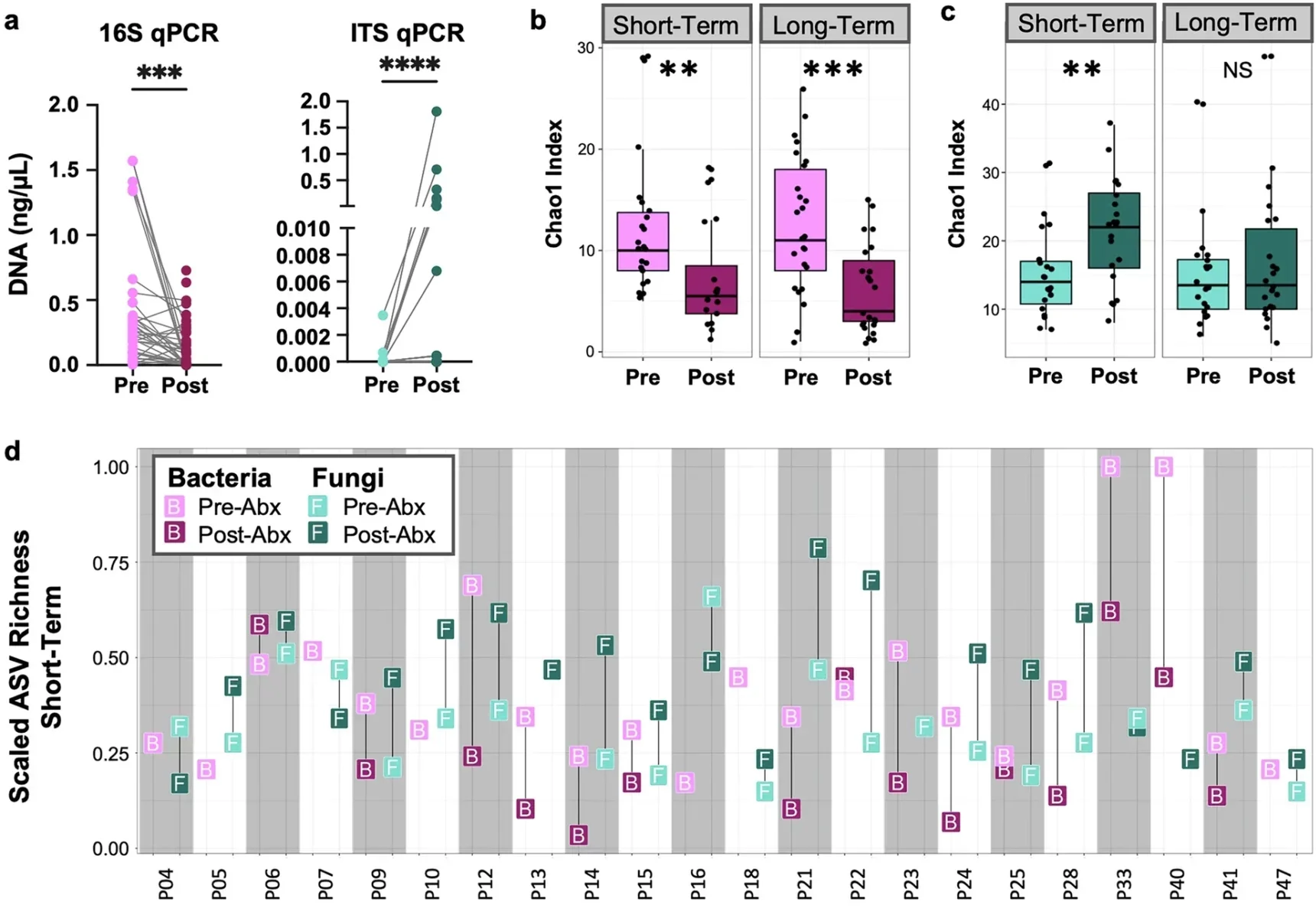
Their ANTIBIO study enrolled 47 infants younger than 6 months who received urgent antibiotic therapy. Twenty-two were treated for two to three days, and 25 for four to 14 days.
Across the cohort, antibiotics reduced bacterial DNA in stool and increased fungal DNA. They also pushed bacterial and fungal diversity in opposite directions. Bacterial richness fell after treatment, while fungal richness rose, especially in the short-term group.
The strongest fungal signal involved Malassezia. After antibiotics, the relative abundance of this genus increased in both short- and long-course treatment groups. The species showing some of the largest fold changes included M. restricta, M. globosa, and M. sympodialis.
The more antibiotics infants received, the more likely Malassezia was to expand. The total number of antibiotics prescribed was the only study variable significantly associated with that increase.
The researchers also found that antibiotics scrambled the usual network of bacterial-fungal relationships in the infant gut. Core bacteria such as Bifidobacterium and Bacteroides lost central roles, while more opportunistic microbes moved into important positions.
That kind of ecological reshuffling may help explain why antibiotic exposure early in life has long been linked to later asthma risk.
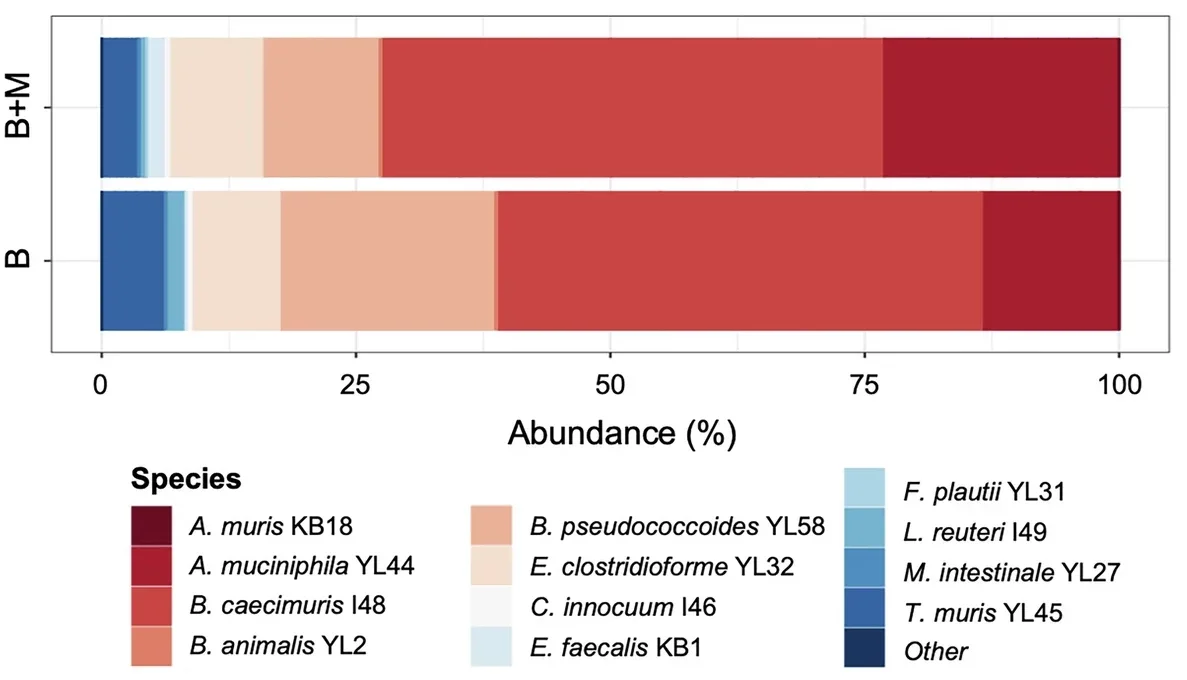
To test whether Malassezia might be doing more than tagging along, Arrieta’s team moved into gnotobiotic mice. These mice are raised with carefully defined microbes.
They focused on M. restricta, one of the fungi that expanded most strongly in antibiotic-treated infants. Even at low levels, the fungus changed the bacterial community in the mouse gut and altered metabolic outputs. Notably, there were reductions in oleate, cortisol, and corticosterone.
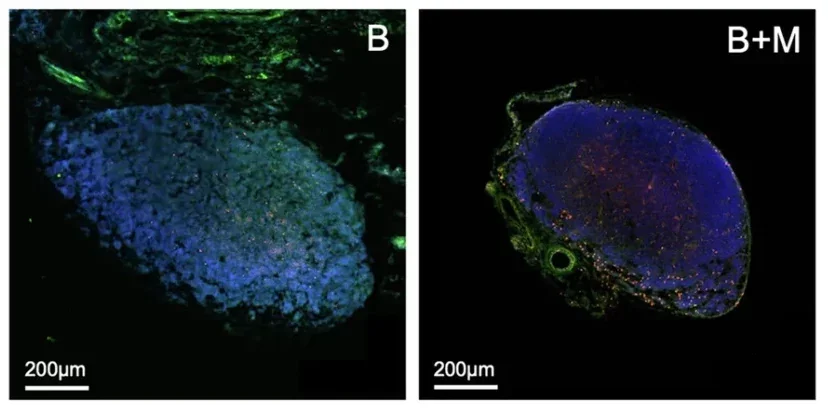
It also changed immune development.
Mice exposed early to M. restricta had higher counts of eosinophils, macrophages, neutrophils, and T helper cells linked to type 2 and Th17 immune responses in the gut and nearby lymph nodes. Some antibody levels in blood also fell.
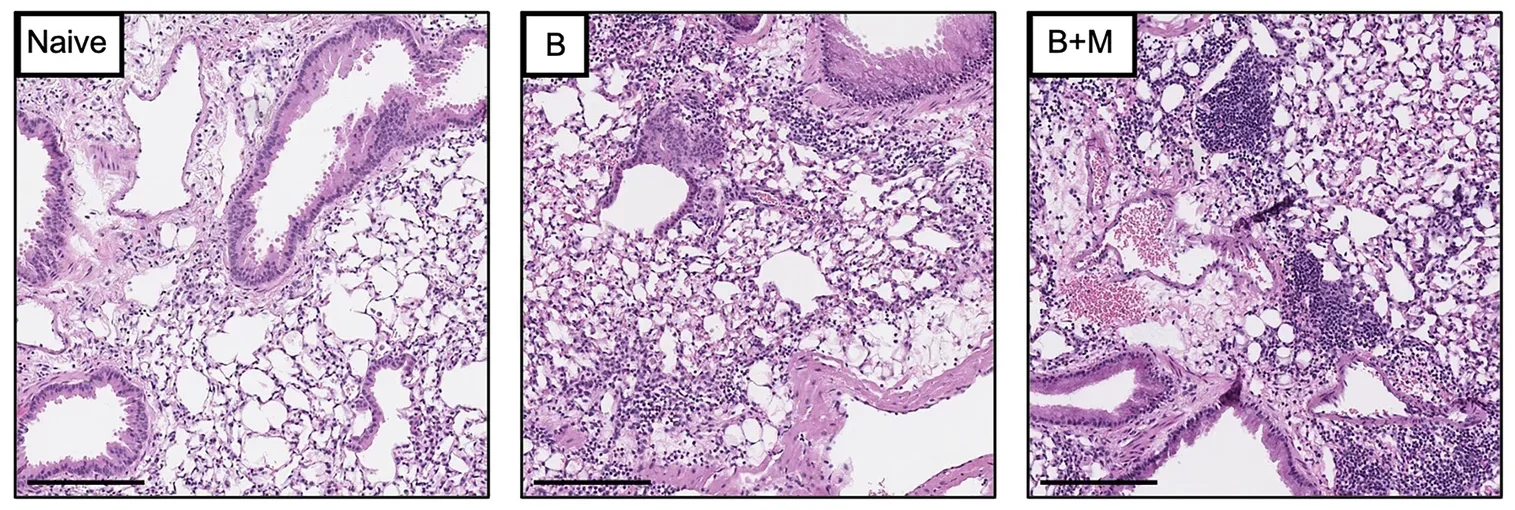
When the animals were later challenged with house-dust mite allergen, those early fungal exposures appeared to matter. Mice colonized with M. restricta developed more severe allergic airway inflammation than mice that carried bacteria alone. In BALB/c mice, the fungus also intensified later allergic inflammation after neonatal infection with respiratory syncytial virus, or RSV.
“These results reveal a previously unrecognized pathway linking early-life antibiotic exposure to allergic disease risk and show how the developing immune system is shaped by fungi within the gut microbiome during a critical window of development,” Arrieta said. “Antibiotics are an essential treatment for young children when needed, but this study shows that there is a previously overlooked effect on the gut mycobiome, allowing species like Malassezia to flourish, and directly impacting immunological function.”
The studies complement each other in a useful way. One identifies fungal patterns associated with later disease in a large human cohort. Moreover, the other offers a possible mechanism, showing how antibiotics can alter the infant mycobiome. The work shows how a rising fungal species may help drive immune changes in animals.
Together, they make a case that the infant gut is not just a bacterial system with a few incidental fungi mixed in. Instead, it is a more complicated microbial environment, and fungi may be important participants in setting immune trajectories early in life.
The authors also stress the limits of what is known. The infant antibiotic study did not include an untreated age-matched control group. It was not powered to sort out the effects of specific antibiotic classes. And mouse models, even carefully designed ones, cannot fully reproduce the complexity of the human microbiome.
The researchers also cannot yet say whether the immune responses they observed are directed specifically at M. restricta, at other microbes shifted by its presence, or at both.
Still, the overlap between the two studies is hard to ignore. Both point to Malassezia as a recurring feature of an immature or disrupted early-life fungal ecosystem. Furthermore, both connect that pattern to immune problems that can show up in the skin, gut, or lungs.
That opens a new line of thinking for pediatric allergy research. If certain fungal patterns can help identify risk early, they might become warning signs. If specific fungi help drive immune dysregulation, they might also become therapeutic targets.
The idea is not to avoid antibiotics when a child truly needs them. The authors are clear that these drugs remain essential. The message is narrower, but important: antibiotics may have broader ecological effects than doctors once appreciated. Some of those effects involve fungi, not just bacteria.
These studies suggest that infant gut fungi may eventually become part of how doctors assess allergy risk, especially after early antibiotic exposure. They also point to the mycobiome as a possible therapeutic target.
Future work will need to confirm whether fungal changes such as rising Malassezia can be tracked reliably in infants.
Researchers also need to confirm whether those shifts directly contribute to disease in children.
In addition, they will ask whether treatments that restore a healthier early-life gut ecosystem could lower the odds of eczema, food allergy, or asthma.
Research findings are available online in the journal Nature Communications.
The original story “Tiny gut fungi could be the key to treating Asthma worldwide” is published in The Brighter Side of News.
Like these kind of feel good stories? Get The Brighter Side of News’ newsletter.
The post Tiny gut fungi could be the key to treating Asthma worldwide appeared first on The Brighter Side of News.


Leave a comment
You must be logged in to post a comment.